
As a dentist, it is my responsibility to diagnose, inform, and treat patients for the dental issues with which they present. However, it can often be a misconception that where that last molar ends, so too does my responsibility to my patients. The mouth is connected to the rest of the body, and it has subtle ways of telling us what’s happening further inward…if you know what to look for. Stomach acid, for example, can erode very hard substances – including TEETH – and if asymptomatic reflux patients aren’t getting help (because they don’t know to be asking for it), dentists might be one of the first clinicians to identify this potentially harmful systemic issue.
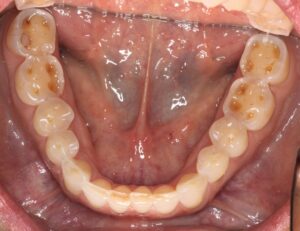
The esophagus connects the stomach to the mouth. Thus, for the 30+ percent of Americans who have some form of reflux, we can assume that their mouth is now directly and intimately connected to their reflux issue. For many reflux patients, gastric acid doesn’t stop at the esophagus and/or larynx; it often spills up into the mouth and leaves behind evidence in characteristic patterns on the teeth (see images below for clinical signs of reflux in the mouth).

Because reflux is linked to esophageal and laryngeal cancers, finding early signs of the presence of acid could be helpful in prevention and early-stage detection efforts.
Screening is difficult in early stages, and prognoses are not great when caught later in the process. While I cannot “see” acid in the mouth, I can see teeth with acid erosion as possibly the one and only sign that my patient may have an undiagnosed issue. These acid-eroded teeth could be the earliest sign for an otherwise asymptomatic patient at potential risk for cancer.
Dentists are “fixers” – when we see a damaged tooth, we immediately start planning our rehab approach. However, I often encourage my colleagues to look at certain types of breakdown (acidic erosion for example) as an opportunity to pause and consider the rest of the body attached to those teeth. In fact, when we rush into treatment of acid eroded teeth, we’ve effectively lost an opportunity for possible early detection, AND our new restorations might be short-lived as they could be the next casualty in the uncontrolled acidic environment. I often compare this to building a sandcastle right at the water’s edge. It might look beautiful during the calm low tide, but as the waters creep back up, that sandcastle will soon be the next victim to the erosive waves. When I lecture to my colleagues about treatment of dental acidic erosion, I stress that restorations should come second to referring patients to their physicians for evaluation and treatment of potential reflux.
Teeth affected by acid erosion can have symptoms of their own. Most notably, root sensitivity as the acid exposes the sensitive inner dentin layer of the teeth. For this reason, palliative treatments are a great way to manage symptomatic patients who are also seeking medical care. Fluoride treatments in the form of in-office varnish or daily use prescription fluoride toothpaste can help by remineralizing the enamel and dentin that are being demineralized by stomach acid. Fluoride is also an excellent desensitizer. Another palliative treatment is smooth surface sealants which serve as a temporary shield from acid washing away more tooth structure (reapplication of the sealant will be necessary if acid continues to present and deteriorate the sealant over time). While the aforementioned therapies can be used intraorally, I also encourage patients to attempt to manage their reflux as well so the teeth are not at risk of an acidic environment. We review diet and I also encourage use of Reflux Gourmet. This alginate therapy creates a temporary barrier to prevent acid from escaping the stomach – and if it is contained – it cannot wreak havoc on any of the vulnerable tissues in its path of destruction.
In my practice, when I see erosion on an asymptomatic patient, I immediately head into a conversation that sounds something like this:
“I’m seeing signs of acid erosion on your teeth. My concern is that if stomach acid is able to eat away at the hardest substance in your body (your teeth), I worry about what it could be doing to the much softer lining of your esophagus.”
I will go on to recommend they speak with their physician and always offer a letter in the event their physician wants to know why the patient has come to them about a problem for which they have no symptoms. MANY patients have returned to tell me that they were diagnosed with reflux are now being treated for it. This has given me the confirmation that these conversations are making a difference – not only in their oral health – but in their overall health.
This article is for informational purposes only. It is not, nor is it intended to be, a substitute for professional medical advice, diagnosis, or treatment and should never be relied upon for specific medical advice. To the extent that this article features the advice of physicians or medical practitioners, the views expressed are the views of the cited expert and do not necessarily represent the views of Reflux Gourmet.
“REFLUX GOURMET” and related trademarks are trademarks of Reflux Gourmet LLC. All material appearing on the Reflux Gourmet website (“content”) is protected by copyright under U.S. Copyright laws and is the property of Reflux Gourmet and/or the party credited as the provider of the content. You may not copy, reproduce, distribute, publish, display, perform, modify, create derivative works, transmit, or in any way exploit any such content, nor may you distribute any part of this content over any network, including a local area network, sell or offer for sale, or use such content to construct any kind of database. For permission to use the content on the Reflux Gourmet website, please contact info@refluxgourmet.com..